Advanced Surgical Management of Perineural Invasion in Head and Neck Cancer Patients
- John Chaplin

- 3 days ago
- 3 min read
Perineural invasion (PNI) presents a significant challenge in the treatment of head and neck cancers. This condition involves cancer cells spreading along nerves, often leading to severe pain and altered sensation. A recent case involving a 76-year-old man with extensive perineural invasion of the left infraorbital nerve highlights the complexity and potential of advanced surgical approaches to manage this condition effectively.
Understanding Perineural Invasion and Its Mechanism
Perineural invasion occurs when cancer cells infiltrate the space surrounding nerves. In head and neck cancers, such as squamous cell carcinoma (SCC), PNI is a known pathway for tumour spread beyond the primary site. This spread can cause symptoms like numbness, tingling, or severe pain due to nerve involvement.
In this case, the patient had a history of SCC on the left cheek skin, removed one year prior. Despite initial treatment, cancer cells spread along the left infraorbital nerve, a branch of the maxillary nerve (cranial nerve V2). The infraorbital nerve runs through the infraorbital canal and exits the skull via the infraorbital foramen, providing sensation to the midface.
Cancer cells travel along the nerve sheath by invading the perineural space, which offers a low-resistance path. This invasion allows the tumor to bypass traditional tissue planes and spread proximally toward the skull base. The involvement of the infraorbital nerve in this patient caused altered sensation and severe pain, indicating significant nerve compromise.
Prognostic Significance of Perineural Invasion
PNI is a critical factor in prognosis for head and neck cancer patients. Its presence often correlates with:
Higher rates of local recurrence
Increased risk of regional and distant metastases
Reduced overall survival
The extent of nerve involvement, especially when it reaches the skull base, worsens the prognosis. Early detection and aggressive treatment are essential to improve outcomes.
Imaging and Surgical Planning
Magnetic Resonance Imaging (MRI) and Positron Emission Tomography (PET) scans played a vital role in assessing the extent of the tumor and planning surgery. In this patient, imaging suggested that the tumour was surgically resectable despite extensive nerve involvement.
The combined expertise of Prof Richard Douglas, a skull base surgeon, and Dr Chaplin, a head and neck and reconstructive surgeon, was essential to address the complex anatomy and achieve complete tumour removal.
Surgical Approach and Technique
The surgical plan involved a two-pronged approach:
Endoscopic Nerve Resection by Prof Douglas
The left infraorbital nerve was accessed endoscopically through the sinuses.
The pterygopalatine fossa, a deep space behind the maxilla, was opened to expose the nerve proximally.
The nerve was transected at the foramen rotundum, where the maxillary nerve exits the skull, separating it from the infraorbital canal.
This approach allowed precise removal of the deepest nerve segment involved with tumor spread while minimizing damage to surrounding structures.

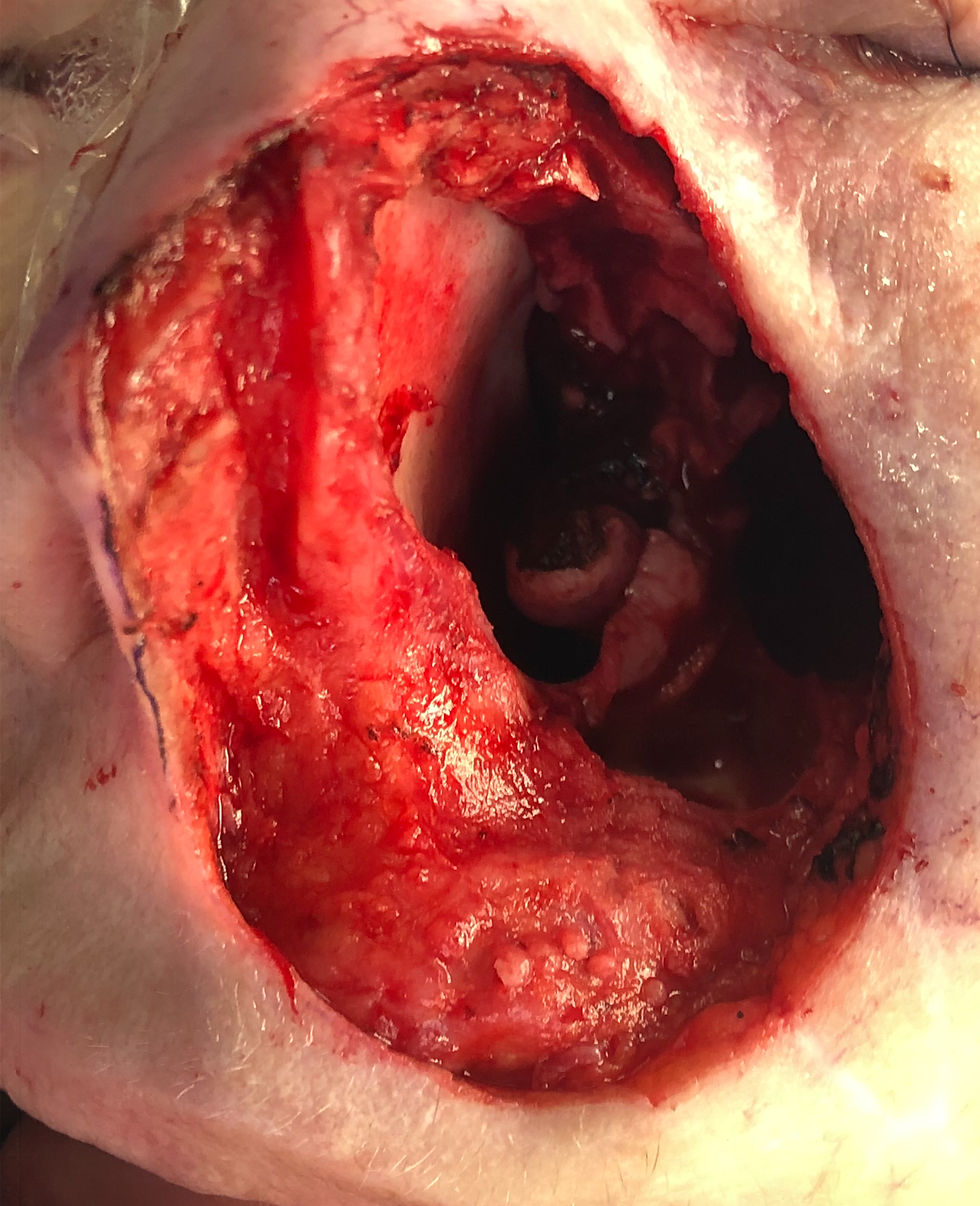
Composite Resection and Reconstruction by Dr Chaplin
Dr Chaplin resected a composite specimen including the cheek skin, anterior maxillary bone, and the involved nerve segment.
The previous local flap used to reconstruct the initial SCC excision defect was also removed to ensure clear margins.
The resulting defect was reconstructed using a radial forearm free flap, a thin, pliable tissue graft with reliable blood supply.
The flap’s pedicle was tunneled through the cheek and anastomosed to the facial artery and common facial vein to restore blood flow.
This complex reconstruction restored facial contour and function, improving the patient’s quality of life after extensive tumour removal.
Key Takeaways from the Case
Early recognition of perineural invasion is crucial for timely intervention. Symptoms like altered sensation and pain should prompt thorough imaging.
Multidisciplinary collaboration between skull base and reconstructive surgeons enables comprehensive tumor removal and functional restoration.
Endoscopic approaches to the skull base and nerve resection reduce morbidity compared to open surgeries.
Free flap reconstruction provides reliable coverage for complex defects after extensive resections.
Imaging techniques such as MRI and PET are indispensable for surgical planning and assessing resectability.
Post operative treatment radiation therapy and or immunotherapy will be indicated as adjuvant treatment for this advanced disease to prevent progression.
Moving Forward with Perineural Invasion Management
This case demonstrates that even extensive perineural invasion involving critical nerves like the infraorbital nerve can be managed successfully with advanced surgical techniques. Patients benefit from a tailored approach that balances oncologic control with functional and aesthetic outcomes.
For clinicians, staying vigilant for signs of nerve involvement and collaborating across specialties can improve patient outcomes. For patients, understanding the nature of perineural invasion and the available surgical options can help in making informed decisions about their care.
If you or a loved one face a diagnosis involving perineural invasion, consult with a specialised head and neck cancer team to explore the best treatment options available.



Comments