
OUR SERVICES
SALIVARY GLAND SURGERY
SALIVARY GLAND SURGERY
Dr John Chaplin – Head and Neck Surgeon Auckland NZ
This article describes indications, techniques and complications of salivary gland surgery. It includes videos of parotid salivary gland surgery performed by Dr John Chaplin, Head and Neck Surgeon in Auckland.
SALIVARY GLAND ANATOMY
There are three paired glands in the head and neck that produce saliva. The parotid glands are the largest and overlie the angle of the jaw in front of the ear. A tube, known as Stensens duct, drains saliva from the glands into the mouth. The openings are inside the cheek opposite the upper molar teeth. The submandibular glands lie deep to the horizontal portion of the lower jaw. The ducts, which are the longest and narrowest of all the salivary glands, enter the mouth under the tongue at the front of the mouth. The sublingual glands lie deep to the lining of the mouth on each side of the tongue, these glands have many short ducts that enter the mouth directly through the lining.
In addition to these major glands there are hundreds of minor salivary glands throughout the lining of the mouth and throat with most on the lips and palate. All of these glands produce saliva in response to food being placed in the mouth. Even the thought or smell of food can stimulate salivary flow and most people make about one litre of saliva per day. As well being 99.5% water, saliva has minerals and proteins that aid digestion and keep the mouth and teeth healthy. There are multiple cell types that make up the tissues of the gland.
SALIVARY GLAND ENLARGEMENT
There are three mechanisms of enlargement of the salivary glands. They are quite distinct and the type of swelling is generally characteristic of the disorder causing it.
REPETITIVE UNCOMFORTABLE SWELLING ASSOCIATED WITH EATING AND DRINKING
GENERALISED NON TENDER SWELLING IN THE SALIVARY GLANDS
This type of swelling usually affects the parotid gland. It involves the whole gland frequently bilaterally and there is no fluctuation, discomfort or association with eating and drinking. There is no inflammation, the gland is generally enlarged, soft, without focal nodularity. The process is called sialdenosis and is associated with certain drugs, alcoholism, aging, obesity and some dieting fads.
FOCAL PROGESSIVE SALIVARY GLAND MASS

This is the typical presentation of a neoplasm in the gland. They are firm, focal, usually solitary nodules within an otherwise normal gland. Tumours most commonly occur in the parotid followed by the submandibular gland. Minor salivary gland tumours are next most common and sublingual tumours are very rare and are nearly always malignant.
Benign tumours are the most common and present as a firm to hard, mobile, regular mass without involvement of overlying or deep structures. They tend to enlarge slowly and progressively and they are painless. Malignant tumours on the other hand can enlarge rapidly, they can become fixed to underlying structures or the subcutaneous tissue and skin overlying the gland. They can involve nerves associated with the salivary gland and can spread to lymph nodes in the neck.
Tumours in the parotid gland are 80% likely to be benign, whereas submandibular tumours are only 50% likely to be non cancerous. In the sublingual gland and minor salivary glands most neoplasms are malignant.
PAROTID SALIVARY GLAND TUMOURS
BENIGN TUMOURS (60%-80%)
These are generally benign tumours of salivary cell origin and are called adenomas. The most common is the pleomorphic adenoma followed by Warthins Tumour (cystadenoma lymphomatosum). They present as a firm mobile mass either in the tail or the preauricular portion of the gland. They can become quite large if left to grow. The majority 90% of these tumours occur in the superficial aspect of the gland (lateral to the nerve) occasionally ,however, these tumours occur in the deep part of the gland, behind the jaw and can even present as a lump in the throat with expansion of an area called the parapharyngeal space. Benign salivary gland tumours cannot cause facial weakness. Pleomorphic adenomas have a risk of malignant change over a long period of time.
CANCER (20%-40%)

The most common malignant tumour (70%) of the parotid gland in New Zealand is metastatic skin cancer (SCC or melanoma) involving intra-parotid lymph nodes. These are highly aggressive tumours that frequently spread to lymph nodes in the neck, and can involve the facial nerve causing partial or total facial weakness. There is usually a history of removal of a skin cancer or melanoma on the scalp, ear, facial or temple skin in the preceding two years.
Occasionally a patient will present with the primary lesion. The mass feels hard and irregular and can be fixed to deep structures or to the overlying skin causing discolouration or ulceration. They can be multiple and there can be palpable lymph nodes in the neck most frequently in the upper deep cervical region (level II). Other malignant primary parotid tumours are more rare and present similarly to benign tumours except that they can cause nerve involvement. They rarely spread to lymph nodes in the neck and progress more slowly than metastatic cancers. They can be hard and irregular to palpation.
SUBMANDIBULAR SALIVARY GLAND TUMOURS

Present as a firm to hard mass within the gland. Usually mobile and will only become fixed and involve nerves (lingual, marginal branch of facial and hypoglossal) if malignant. Skin cancers and melanoma can spread to nodes in this region also, however the lymph nodes are not within the substance of the gland like the parotid gland but attached to the fascia around the gland. They are usually associated with the facial artery.
SUBLINGUAL SALIVARY GLAND TUMOURS
Uncommon and usually malignant (75%-100%). Present as a hard mass in the floor of mouth and can often involve the lingual nerve causing numbness in the floor of mouth and tongue. Rarely spreads to neck.
MINOR SALIVARY GLAND TUMOURS
Uncommon and more likely (50%-80%) to be malignant. Present as a submucosal lump on the oral or nasal mucosa. Most common on the palate, lip, tongue and floor of mouth.
INVESTIGATIONS
Clinical assessment is very important in the diagnosis of salivary gland masses. Investigations are not always necessary and in fact can lead to a false sense of security and adoption of conservative management when surgery is required. There is however a role for investigating some parotid and other salivary gland tumours.
TISSUE BIOPSY
The single most important investigation and the method depends on the site of the tumour.
-
Fine Needle Aspiration Biopsy – used in parotid, submandibular, parapharyngeal space tumours. This test has an accuracy of 80-95% and there is no documented risk of seeding tumour along the needle track (unlike large needle core biopsy). The needle biopsy can help in the diagnosis and also help plan the type of operation required. There is a risk of false negative results for malignancy and results should be considered with the clinical presentation.
-
Open biopsy – used in minor salivary gland and sublingual tumours. Incisional or excisional depending on the size of the lesion. Accurate because tissue architecture is seen as well as cells.
IMAGING
Ultrasound is useful in superficial parotid lesions (the majority) and the submandibular gland. It can help tell wether a lesion is within the gland and whether a lesion is cystic or solid.
CT scan is useful in the parotid if the lesion is large, involves the deep lobe or parapharyngeal space and particularly if it is malignant and there is a risk of lymph node involvement. Useful in minor salivary tumours particularly in the palate and for sublingual tumours which are not able to be imaged with ultrasound. The best test for recurrent submandibular gland swelling with no obvious stone in the duct.
MRI Scan can also be useful in sublingual tumours where dental amalgam may distort CT images and multiple planes of imaging are required.
Sialography Not useful for investigation of tumours but useful in recurrent gland swelling where there is no obvious stone and either a small stone or stricture suspected.
Plain Xray (occlusal and oblique views) useful only for recurrent swelling where there is a suspected stone or multiple stones in the duct.
TREATMENT
(For management of sialadenitis see article on salivary stones.)
Surgery is required for all salivary tumours with the only exceptions being a probable benign tumour in an older patient who is reluctant for surgery or is an anaesthetic risk. Even with a tumour that is suspected to be benign on investigation the rationale for operating is threefold. 1. All tumours progress and the risk to the surrounding structures are greater with larger tumours. 2. It can be difficult to diagnose malignancy clinically and there is a false negative rate with needle biopsy. 3. Benign salivary tumours are at risk of malignant transformation.
Parotid Salivary Gland Surgery (Parotidectomy)
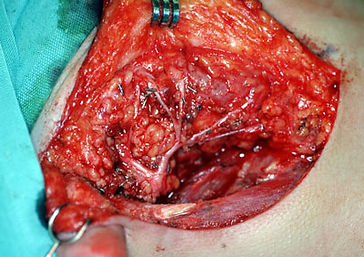
The operation is performed under general anaesthetic. An incision is made in front of the ear it passes down behind the ear lobe and then curves forward into the neck. It is a similar incision to that used for a cosmetic facelift it heals well and is rarely noticeable. The wound is carefully closed at the end of the operation and a suction drain is placed to remove any blood or fluid that would otherwise collect under the skin.
The operation varies depending on the type, position and size of the tumour. For the majority of parotid tumours only a portion of the gland containing the tumour is removed. If the tumour involves the deep lobe, is large or is metastatic skin cancer in parotid lymph nodes the majority of the gland is removed. With some deep lobe parotid tumours the jaw needs to be opened to allow access to the deep part of the tumour. Occasionally and only with advanced malignant tumours the facial nerve needs to be removed.
With metastatic skin malignancy and some high grade salivary cancers where lymph nodes are involved removal of neck lymph nodes is also necessary. This operation is called a neck dissection and is described in the article on Neck Dissection.
POSSIBLE COMPLICATIONS
It is important to be aware that the complications described are rare particularly when the surgeon does this operation regularly.
FACIAL NERVE INJURY
The key to Parotid salivary gland surgery (parotidectomy) is finding and preserving the nerve that supplies muscle function to each side of the face. The facial nerve runs right through the parotid gland and is usually in contact with the capsule of the tumour somewhere. Temporary weakness of a portion of the face is more common but permanent weakness of the entire face is very rare particularly in benign tumours. With advanced cancers occasionally a portion or the entire nerve needs to be sacrificed to get clearance of the tumour this is never the case in benign tumours. The risk to the nerve is much higher in recurrent parotid surgery.
SENSORY NERVE INJURY
The great auricular nerve runs through the back of the superficial part of the parotid and can usually preserved. Removal of this nerve is sometimes necessary and this resukts in numbness of the earlobe and also the skin of the cheek overlying the parotid. If the nerve is only bruised this will usually recover.
HAEMATOMA
Bleeding into the operative site requires a return to the operating theatre, removal of the blood clot and ligation of the bleeding vessel.
SALIVARY LEAK
Because some of the parotid gland is usually left behind after the operation, saliva can leak from this into the wound. The saliva either causes a small collection or can leak from the wound edge. This usually stops on its own but a drain can be put into the wound to help settle the leak.
FACIAL SWEATING (FREYS SYNDROME)
In the months to years after parotid surgery some patients can develop sweating from the skin over the parotid area. This is due to nerves from the gland growing into the sweat glands. It is not common for this to be problematic. There are a number of treatments available but the best is botox injection into the overlying skin.
PAIN
Parotidectomy does not tend to be a very painful operation. There can be some discomfort on mouth opening and chewing in the days following surgery but this is usually controlled with simple pain medication like Panadol.
Post operatively one to two nights in hospital are required and normal activities can be resumed in one to two weeks.
Submandibular Salivary Gland Surgery
This operation is also best performed under general anaesthetic. The incision is made in the neck about two finger breadths below the lower border of the jaw in a skin crease. The wound usually heals very well and after a period is almost imperceptible. A drain is also used in this operation.
The entire gland is removed also with a small portion of the duct. If there is a malignant tumour a wider excision is often required with removal of surrounding soft tissue or jaw bone including muscle, lymph nodes and occasionally surrounding nerves. In metastatic skin malignancy and some high-grade salivary cancers with lymph node involvement removal of lymph nodes in the neck is also necessary. This operation is called a neck dissection and is explained in another article.
POSSIBLE COMPLICATIONS
It is important to be aware that the complications described are rare particularly when the surgeon does this operation regularly
NERVE INJURY
There are three nerves at risk.
The Marginal Branch of the Facial Nerve supplies muscle function to the lower lip and is most at risk during this operation. If the nerve is stretched or cut the lower lip can be weak and the smile crooked. This is uncommon and if it occurs at all it is unlikely to be permanent
The Lingual Nerve supplies sensation to the floor of mouth and side of the tongue. Numbness of these areas will occur if the nerve is cut. This is very rare.
The Hypoglossal Nerve supplies muscle function to the tongue. If injured the tongue can be paralysed on one side. This is extremely rare.
These nerves are more likely to be permanently damaged if the tumour is cancerous and has spread into surrounding structures.
HAEMATOMA
Bleeding into the operative site requires a return to the operating theatre, removal of the blood clot and ligation of the bleeding vessel.
INFECTION
This complication is very rare in clean head and neck surgery.
RANULA
It is possible following submandibular gland removal to traumatise the sublingual gland and for this to develop a leakage of saliva into the neck. This is rare and would be treated by removal of the sublingual gland.
Post operatively one to two nights in hospital are required and normal activities can be resumed in one to two weeks.
MINOR SALIVARY GLAND SURGERY
This operation is also best performed under general anaesthetic. The incision is made in the neck about two finger breadths below the lower border of the jaw in a skin crease. The wound usually heals very well and after a period is almost imperceptible. A drain is also used in this operation.
The entire gland is removed also with a small portion of the duct. If there is a malignant tumour a wider excision is often required with removal of surrounding soft tissue or jaw bone including muscle, lymph nodes and occasionally surrounding nerves. In metastatic skin malignancy and some high-grade salivary cancers with lymph node involvement removal of lymph nodes in the neck is also necessary. This operation is called a neck dissection and is explained in another article.
SUBLINGUAL SALIVARY GLAND SURGERY
Sublingual gland tumours are rare, usually malignant and require aggressive surgical treatment. Sublingual salivary gland surgery can often be performed through the mouth but sometimes opening or even removal of part of the jaw is necessary to get access. A neck incision is also frequently required to get clear margins and remove lymph nodes in the neck. The Lingual and Hypoglossal Nerves are frequently involved and these often need to be removed. This is not the case when the sublingual gland is removed for benign conditions such as Ranula.
If a large area of soft tissue is resected from the floor of mouth sometimes this will need to be reconstructed with tissue brought in from other parts of the body such as skin from the forearm. In this situation there will often need to be a period of tube feeding while the tissues heal.